My Morning Medications Round (mis-Adventure in Aged Care)
CPDTime.
7m
Updated 30 Jun 2024
It's reported that a common cause of medication errors is interruption and/or distraction to the nurse during the medication round (Raban et al. 2013).
We can’t stop interruptions, and aiming for zero medication errors seems like a tall order.
As an example, let's consider some of the potential causes for medication errors that can (and do) occur in a wandering dementia ward with, say, 14 residents. (Note: The medications referred to in this scenario do not include S4s or S8s.)
The 0730 hour round requires the RN or EN to administer/instil/inject/insert approximately 84 medications - an average of 6 per resident, be it insulin, eye drops, tablets, suspensions, inhalers or suppositories.
For Starters:
The medication charts are placed in the large medications folder in order of the room numbers as you traverse the corridor - but there's just one problem: many residents are already up and about. So, do I search for them, now pushing the trolley, or wait until I come across them on my travels, and end up totally out of sync with my medication charts?
Resident Nellie, who has already been in the garden, approaches me with a bunch of greenery she has snapped off from the tips of plants or branches - rosemary, bottle brush or geranium - and I dare not refuse her kind gesture. I learnt ages ago to carry a plastic tumbler on the trolley top for such occasions. I've got you now, Nellie, how about your eyedrops whilst we stand in the corridor? 'No thank you dear, you have them...' she replies as she breaks from my gentle grasp on her arm, wandering off. There will be another opportunity soon.
Resident Jack is next. He sees me coming and makes a beeline for his room, thinking he can fool me as he enters the shared ensuite and exits the other resident's bedroom door - only to re-enter the corridor closer to me. His fear is that I am giving him dementia in the form of a pill and keeping him here against his will. No amount of explanation can convince him that the 'D' in Vitamin D does not stand for dementia. I spend two minutes just on this one pill, and I still have to give him another five.
The DECT phone rings continuously, alerting me to a resident's call bell (which at this stage I am not required to attend) or an 'assist call' (which I do have to attend to). Additionally, outside calls are coming in as the only administration officer has yet to start work to take such calls. And furthermore, the ENs in other wings are calling to ask me to authorise PRN paracetamol tablets.
….and so it goes on.
About 1 ¼ hours later I return with my trolley to store it in the pharmacy, the medication charts infused with the aroma of rosemary or mint. Only one more pill round for my shift; thankfully, the lunchtime medications aren’t as many. I can delegate this round, as most days I have another adventure to embark on.
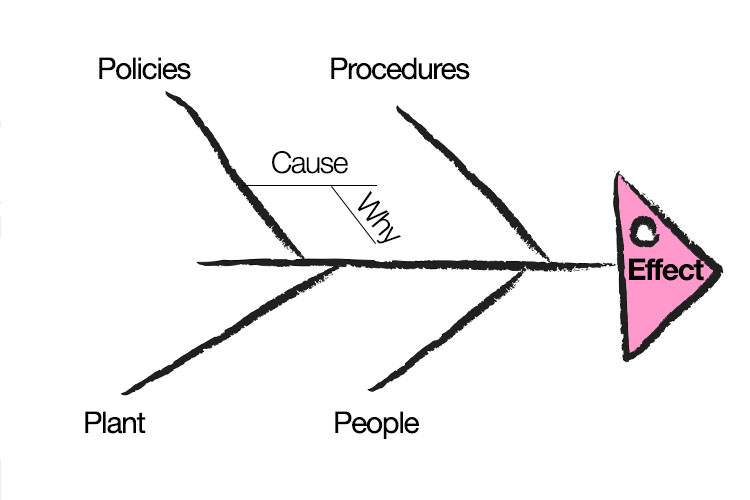
The Cause and Effect (a.k.a. ‘Fishbone’) Diagram.
How Can We Ensure That All Prescribed Medications Have Been Given?
In the quietness of the pharmacy, go through the charts, making sure you have given and signed for all medications. (You may have given Resident Frank all of his pills, but as you were signing for them, another resident approached wearing his PJ top only. Do you call for another staff member to help, or attend to Frank yourself? The distraction may have caused you to not complete the signing).
Towards the end of your shift, ask a colleague to again check your charts, and you check theirs.
Think about the pros and cons of purchasing 'Do not interrupt me' vests.
Finally, on pharmacy pre-packed pill dispensers: I have found that they are useful in facilities where the care staff administer some medications, but who remain unaccountable for what the pharmacist placed in the packs. However, as a registered nurse, I preferred to administer straight from the bottle/packet, as I found it difficult to recognise/identify each pill by its colour, shape and/or markings in a time-efficient manner, and I was accountable for the pills I administered.
Interruptions and distractions are just one of the many causes of medication errors that the aged care nurse has to contend with.
Consider:
The resident who is required on this first morning round to take his medications on an empty stomach.
The residents with varying degrees of dysphagia and what the nurse has to watch for before they are satisfied the pills have been safely swallowed.
The resident who is a master at hiding the pills somewhere in their mouth, only realised sometime later when spat-out pills are found in the bed linen or on the floor.
No doubt there are readers out there thinking, 'Well, just change the medication round time, provide breakfast earlier/later, trial a new start time for the AM shift', and so on. However, it's not that easy, because a lot of interdepartmental and employee consultation has to happen prior to implementing such changes, and if it does - well and good.
In the meantime, however, managers: allow sufficient time in the list of daily duties for your staff to spend the time it takes to safely administer medications to groups that take time, especially the residents with wandering dementia; or residents with dysphagia associated with ageing and dementia; or those you need to wake, sit up, wash their faces and give them a drink to ensure they are alert enough to take their pills.
I cannot expect that the care staff have all their allocated residents wide awake, bright-eyed and bushy-tailed within the first hour of their shift.
Additionally, managers: every quarter, print off your list of logged medication errors, and with your staff, utilise any of the quality tools that will help identify the many causes of these errors. Interruptions are just one cause.
A good tool, for example, is the 'Fishbone' or 'Cause and Effect Diagram' (above), as it will provide you and your team with the opportunity to brainstorm the main causes and sub-causes of these errors, thus revealing areas to be targeted.
On a lighter note, there are many adventures in aged care - not just the medication round. Dealing with residents' little peculiarities, warming to their endearing qualities, knowing how much they depend on me and how much pleasure (and the odd laugh) they give me… I wouldn't have it any other way.
 New
New