Although we tend to throw around the term 'congestive heart failure' like there is such a beast, the truth is that there are scads of pathophysiologic differences between left and right CHF, low- and high-output CHF, and systolic and diastolic CHF. It is also essential to understand that the signs and symptoms that signal congestion are quite different from those that signal low cardiac output or perfusion.
Left v Right Congestive Heart Failure
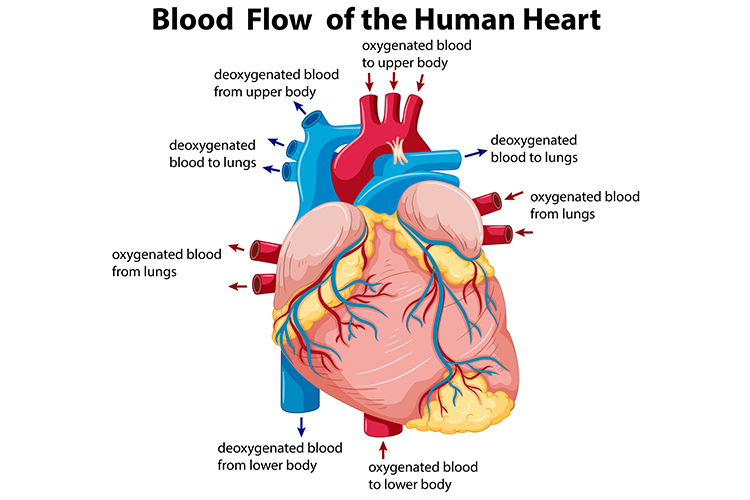
Heart failure (HF) is typically described as left or right HF, which is somewhat simplistic since the functions of the left and right ventricles are inextricably intertwined. However, the terminology is still useful since it points out which ventricle (left or right) is primarily affected.
In left HF, the left ventricle fails, defaulting on its duties as a pump to the periphery. The patient is left with a highly ineffective blood transport system for the body.
In right HF, the right ventricle is the chief culprit. Blood does not flow properly to the lungs; this results in a reduction in gas exchange in the alveoli. Pulmonary hypertension in left heart disease (PH-LHD) is the most common form of pulmonary hypertension (Mehra et al. 2019).
To make things worse, the chaotic flow of blood then travels from the lungs to the left ventricle, where it produces a suboptimal pre-load, making it quite difficult for the left ventricle to eject a useful volume.
Think on it. These are two vastly different problems necessitating two vastly different treatment protocols… yet they both lead to a single endpoint: heart failure.
Low v High Output Heart Failure
Most HF patients have a low - or, at best, a normal - cardiac output. This reduction in output is created by a ventricle that is incapable of ejecting a proper volume of blood, either because of damage to the ventricle itself or because of a poor pre-loading stage. This low output can be present during exercise or - in the most heinous cases - at rest.
However, some patients can suffer the same symptoms and signs of HF without this reduction in load. This less-common condition has been labelled 'high-output heart failure'. Typically, this is caused by an underlying condition such as pregnancy, chronic anaemia, sepsis or hyperthyroidism. High-output heart failure is produced when there is a reduction in the vascular resistance of the body (caused by vascular vasodilation or other factors), which leads to a fall in arterial blood pressure (Cerit et al. 2017).
It should be obvious that many of the normal medications used to help HF patients can’t be used in high-output patients. ACE inhibitors, beta-blockers (with vasodilatory properties) and other medications commonly used to support cardiac function can only worsen the problem by further reducing systemic vascular resistance.
Think of it like this: the 'pipes' are opened wide, and the heart cannot maintain adequate pressure to the body. However, diuretics and dietary restrictions of water and salt are appropriate and are commonly prescribed.
Systolic v Diastolic Heart Failure
One of the first steps necessary in the management of CHF is to assess the underlying pathophysiology.
An easy way to remember the difference is that a heart with systolic dysfunction suffers from an inability to contract, whereas a heart with a diastolic dysfunction suffers from an inability to relax. Note that most diastolic dysfunction is typically referred to as 'preserved systolic function'.
Systolic dysfunction is much easier to diagnose than diastolic dysfunction. In order to accurately diagnose diastolic dysfunction, Doppler echocardiography must be employed, a procedure that is technically difficult to perform and complicated to interpret (Jentzer et al. 2017).
Patients with preserved systolic function are generally older, female, less likely to have certain risk factors (smoking, coronary artery disease, history of myocardial infarction) and more likely to have others (hypertension).
Up to half of all heart failure patients have a preserved systolic function, yet there is little guidance in literature on how to best treat these patients (Abbate et al. 2015). Studies do stress how important it is to differentiate between the two. The medications of choice for each condition are quite varied, and some therapies for systolic dysfunction would be inappropriate and even detrimental if used for a patient with preserved systolic function.
Signs and Symptoms of Heart Failure
The signs and symptoms of heart failure can be divided into those that signal congestion and those that signal low cardiac output or perfusion (see charts). Symptoms like dyspnea (difficulty in breathing), orthopnea (shortness of breath when lying flat) and paroxysmal nocturnal dyspnea (a severe increase in shortness of breath caused by the volume shift from the legs to the chest that occurs after 30+ minutes lying supine) are hallmarks of CHF.
In fact, some physicians will ask patients to use terms such as 'two pillow' or 'three pillow' orthopnea to differentiate how severe their congestion is.
Rapid weight gain - 2 to 3 lbs in 24 hours or 5 lbs in a week - and ankle oedema are readily observable signs taught to patients to help them know when to seek immediate medical attention (American Heart Association 2022).
What about signs of poor cardiac output? Excessive fatigue and poor exercise tolerance can serve as neon signposts pointing to low cardiac output or perfusion. They are often the first symptoms noticed by patients, even prior to receiving a diagnosis of CHF. It is because of these factors that patients lose function and start to self-limit activity. Notably, these symptoms respond well to regular exercise.
Signs and Symptoms of Congestion
|
Signs and Symptoms of Poor Perfusion/Low Cardiac Output
|
Not all patients with CHF will manifest all these signs and symptoms, but almost all of them will demonstrate these hallmarks:
- Shortness of breath or trouble breathing
- Excessive fatigue, especially with exertion
- Swelling in the ankles, feet, legs, abdomen and veins of the neck.
Conclusion
The population is trending older, and with that age comes a price. Hypertension, coronary artery disease, renal disease and other conditions pave a clear path for the onset of heart failure. Sadly, despite massive advances in diagnosis, therapy, and prognosis, the clinical pathway for most patients with heart failure continues to be one of 'inexorable decline'.
Topics
References
- Abbate, A et al. 2015, ‘Heart Failure With Preserved Ejection Fraction: Refocusing on Fiastole’, International Journal of Cardiology, vol. 179, viewed 7 December 2023, http://www.sciencedirect.com/science/article/pii/S0167527314022670
- American Heart Association 2022, Self-Check Plan for HF Management, AHA, viewed 7 December 2023, https://www.heart.org/-/media/Files/Health-Topics/Heart-Failure/HF-Symptom-Tracker.pdf
- Cerit, L, Kemal, H, Gunsel, A, Duygu, H 2017, ‘High-Output Heart Failure: With or Without Obesity’, Journal of the American College of Cardiology, vol. 69, no. 1, viewed 7 December 2023, https://www.jacc.org/doi/full/10.1016/j.jacc.2016.08.080
- Jentzer, JC, Mankad, S, Pislaru, S, Barsness, G, Kashani, K, Rabinstein, A & White, R 2017, ‘Diastolic Dysfunction by Doppler Echocardiography Predicts Mortality After Cardiac Arrest’, Journal of the American College of Cardiology, vol. 11, no. 69, viewed 7 December 2023, https://www.infona.pl/resource/bwmeta1.element.elsevier-04e3c000-224a-3d2f-8f05-19bde95c499a
- Mehra, P et al. 2019, ‘Pulmonary Hypertension in Left Heart Disease’, Archives of Medical Science, vol. 13, no. 1, viewed 7 December 2023, https://www.archivesofmedicalscience.com/Pulmonary-hypertension-in-left-heart-disease,65206,0,2.html